Internship assessment
My internship started started with unit duty
 Grades of hepatic enchephalopathy
Grades of hepatic enchephalopathy

In 1 and 2 week these are the blogs I have done
With detailed history and examination
http://52-santoshkumar.blogspot.com/2022/12/65-yr-old-male-patient-with-soband.html
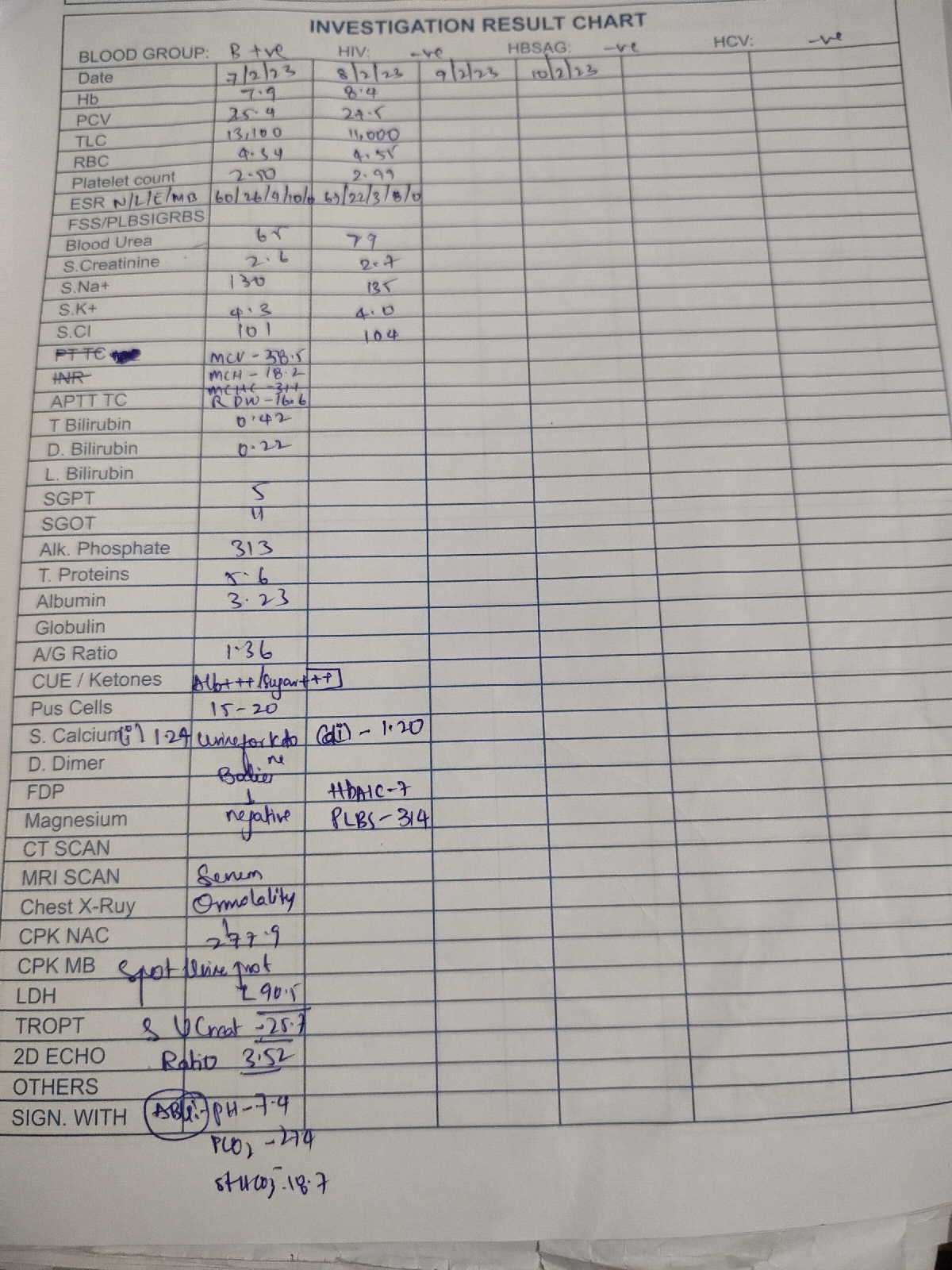
This is a case of
CHRONIC DECOMPENSATED LIVER DISEASE WITH HIGH SAAG LOW PROTEIN ASCITES SECONDARY
TO ALCOHOLIC LIVER DISEASE WITH B/L LOWER LIMB EDEMA GRADE 2 WITH HYPONATREMIA AND HYPOKALEMIA here in this case
I learned per ABDOMINAL examination in detail
New learning points
Grades of ascites
Grade 1 clinically inevident ascites but by ultrasound
Grade 2. Moderate ascites with symmetrical abdominal DISTENSION with flanks fullness
Grade 3 large or gross abdominal DISTENSION
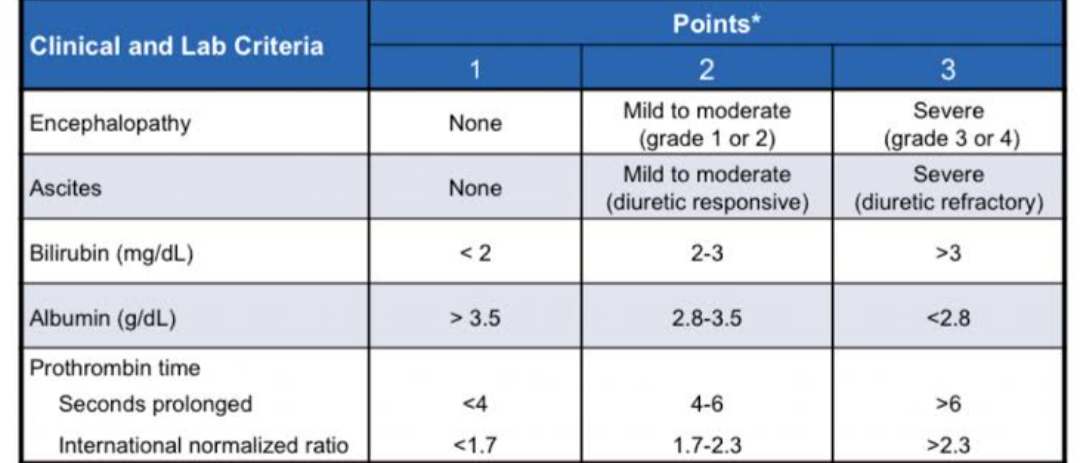
Child Pugh score for portal hypertension
http://52-santoshkumar.blogspot.com/2023/01/60-yr-old-female-with-headache-and-neck.html
Here this female complaints symptoms similar to Rheumatoid arthritis
New learning points
Other systemic disorders associated with rheumatoid arthritis
CVS. Pericarditis
Hematology Feltys syndrome. Neutropenia + splenonomegaly+ RA
RS. Pleural effusion
GI. Mesenteric ischemia due to vasculitis
http://52-santoshkumar.blogspot.com/2022/12/40-yr-old-female-presented-in.html
This is the 1 St death case I have seen in unit duty
Pt came with altered sensorium which later progressed to coma
I learned different stages of coma
Next I was posted in nephrology department
In nephrology department
I used to took some histories of patient and how they landed in this condition
One of the history is
60 year old female came to casualty with complaints of swelling of legs and sob from 15 days
She was apparently asymptomatic 15 days ago.
-she is experiencing SOB on exertion since 15 days which has been progressive (didn’t relieve with diuretics)
- pedal edema and facial puffiness since 15 days
- H/o abdominal DISTENSION
- H/o decreased urine output
-H/o low back pain since 3 years
- h/o NSAID use
No history of orthopnea and paroxysmal nocturnal dyspnea
No history of fever, vomiting,pain abdomen,loose stools,chest pain, palpitations.
Past history:
Diagnosed with diabetes since 15 years and on Inj HAI 4U TID
Hypertension since 20 years, on amlodipine 10mg.
- H/o gynecological surgery .
Diagnosis - Renal failure secondary to NSAID use
Know case of Dm2 and HTN
My learning points
How NSAID will cause renal failure and other causes of renal failure
In ICU my workings are
ICU duty:
Monitored vitals of all the patients in ICU and AMC
I have inserted Foleys ,ryles tube to some patients
I assisted pgs in inserting central cannula
I have inserted iv cannula to many patients and monitored pt during blood transfusion
My learning points
1 how to check pulses paradoxes
2 heared S3 heart sound in heart failure pt ( how to recognise )
3 treating pt with liver failure and heart failure
learned to took abg samples
From radial artery
Later I learned taking abg from brachial artery and
Femoral artery
Ward duty
Here I conducted prefinal examination practical for final year student
Learning points ( learned during taking viva for students)
1 examination of respiratory system indetail
2 difference between type 1 and 2 respiratory failure
3 how to approach a case / diagnosing a case based on only clinical history
4 asking negative history to rule out other differentials
5 treating a case of epilepsy
Unit duty in last 15 days
http://52-santoshkumar.blogspot.com/2023/02/68-yr-old-male-with-intermittent-fever.html
This is a pt diagnosed as ANEMIA UNDER EVALUATION SECONDARY TO ? GI blood loss associated with infection
K/C/O DIABETIC NEPHROPATHY SINCE 2 YEARS
K/C/O OSA SINCE 3 YEARS
Learning points
I learned how to diagnose gi blood loss clinically
Role endoscopy and colonoscopy in diagnosing gi blood loss
I took samples of stool and urine to know progression and cause of blood loss
http://52-santoshkumar.blogspot.com/2023/02/34-yrm-with-compressive-myelopathy.html
This was a case of compressive MYELOPATHY
Learning points
CNS examination in detail
How to diagnose compressive MYELOPATHY by reading MRI
How to treat this patient
My CNS examination that I have done in detail
CENTRAL NERVOUS SYSTEM EXAMINATION-
Higher mental functions
- Conscious
- Oriented to time,place and person
- Memory - Intact
- Speech - no deficit
Cranial nerve examination
• 1 - olfactory sense - normal
• 2- Direct and indirect light reflex present
• 3,4,6 - no ptosis and nystagmus
All eye movements were normal
• 5- Touch -
Sensory -by cotton and pin felt
Motor - chewing movements seen
• 7- no deviation of mouth, no loss of nasolabial folds, forehead wrinkling present
• 8- Hearing normal
• 9,10- position of uvula is central
No regurgitation after drinking water
• 11- looked for trapezius muscle - contraction present
• 12- no deviation of tongue on protrusion
Motor system
Attitude - left and right lower limb slightly flexed at knee joint in lying down posture
Reflexes
Right Left
Biceps - -
Triceps - -
Supinator - -
Knee. . +3 +2
Ankle. +2. +2
Babinski. B/L extension of great time is seen
Power
Upper limb -5/5
Lower limb -5/5
TONE. Lt. Rt
Upper limbs N N
Lower limbs N N
No involuntary movements
SENSORY SYSTEM
I – SPINOTHALAMIC R L
1. Crude touch N N
2. Pain. N. N
II – POSTERIOR COLUMN
1. Fine touch. N. N
2. Vibration sense not felt on Lt lower limb but it slightly felt on rt lower limb
3. Position sense. N. N
4. Romberg’s sign - positive
III – CORTICAL
1. Two point
discrimination.
2. Tactile localisation. Not localised at some points and he delayed to localise the point at other regions in both lower limbs
3. Graphaesthesia. N. N
4. Stereognosis. N. N
Finger nose Coordination present
No dysdiadokinesia
Knee heel coordination present
Gait. Appear to be normal
Swaying seen when he walks on narrow path
And discomfort seen while walking down stairs
http://52-santoshkumar.blogspot.com/2023/02/65-yr-old-female-with-involuntary.html
This a case of hyper glycemia with chorea
Learning points
How hyperglycemia will cause chorea ? What is the pathogenesis
Difference between HHS and diabetic keto acidosis
Acute and chronic complications of diabetes
Types of DM
Diabetic nephropathy stages
During OP days and other works ihave done are
I learned to take history for different cases
I have seen a case of facial nerve palsy and I diagnosed it as LMN type
Sending appropriate investigations for diagnosis
Collecting report s , updating fever chart , updating glucose trends
https://youtu.be/8TW-n6UAJ5o
PSYCHIATRY DUTY :
learnt about the importance of history taking and cases like
ALCOHOL DEPENDENCE SYNDROME
TOBACCO DEPENDENCE SYNDROME