34 yr/M with COMPRESSIVE MYELOPATHY
February ,2023
 MRI cervical spine with whole spine screening
MRI cervical spine with whole spine screening



This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : SANTOSH KUMAR .K ( Intern )
Roll Number : 62
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Chief compliants
34 yr old male ,autodriver by occupation presented with c/o weakness of left lower limb since 3 months
Tingling sensation of left foot since 2 months
HOPI
Pt was apparently asymptomatic 7 months back then he noticed weakness in his left lower limbsb insidious onset , gradually progressive associated with decreased sensations since past 3 months and tingling sensation of left foot since 2 months
He went to neurosurgeon on 24/8/2022 and was advised MRI dorsal spine which was normal .pt complaints did not resolve and he came to our hospital now
H/o difficulty in gripping his foot wear
H/o difficulty in getting up from squatting position
H/o difficulty in climbing upstairs and downstairs
No H/o involuntary movements
H/o head trauma 10 yrs back (not associated with loss of consciousness , vomiting)
NoH/o LOC, memory loss,loss of smell, decreased vision, difficulty in chewing , deviation of mouth , dribbling of saliva
No H/o diplopia ,loss of hearing,hoarseness of voice
NoH/o deviation of tongue
H/o swagging positive
No H/o bowel and bladder incontinence
NoH/o fever, vomiting ,headache
Past history
Not a know n case of epilepsy ,HTN ,T2DM ,CAD,CVA,ASTHMA, THYROID DISORDER.
Personal history
DIET- mixed
Appetite: Normal
Bowel and bladder movements are regular
Sleep: adequate
No allergies
Occasional alcoholic
General examination
Pt is conscious , incoherent, co-operative
No pallor
Icterus
Cyanosis
Clubing
Lymphadenopathy
Edema
Vitals
BP 110/70mmhg
PR 76 BPM
RR 18 cpm
Spo2 98
Grbs. 108 mg/ dl
Systemic examination
Respiratory examination
BAE +ve and normal vesicular breath sound heard
No crepts heard
CVS examination
S1S2 heard
No murmurs heard
Abdomen examination
Soft non tender
No hepatomegaly and splenomegaly
CENTRAL NERVOUS SYSTEM EXAMINATION-
Higher mental functions
- Conscious
- Oriented to time,place and person
- Memory - Intact
- Speech - no deficit
Cranial nerve examination
• 1 - olfactory sense - normal
• 2- Direct and indirect light reflex present
• 3,4,6 - no ptosis and nystagmus
All eye movements were normal
• 5- Touch -
Sensory -by cotton and pin felt
Motor - chewing movements seen
• 7- no deviation of mouth, no loss of nasolabial folds, forehead wrinkling present
• 8- Hearing normal
• 9,10- position of uvula is central
No regurgitation after drinking water
• 11- looked for trapezius muscle - contraction present
• 12- no deviation of tongue on protrusion
Motor system
Attitude - left and right lower limb slightly flexed at knee joint in lying down posture
Reflexes
Right Left
Biceps - -
Triceps - -
Supinator - -
Knee. . +3 +2
Ankle. +2. +2
Babinski. B/L extension of great time is seen
Power
Upper limb -5/5
Lower limb -5/5
TONE. Lt. Rt
Upper limbs N N
Lower limbs N N
No involuntary movements
SENSORY SYSTEM
I – SPINOTHALAMIC R L
1. Crude touch N N
2. Pain. N. N
II – POSTERIOR COLUMN
1. Fine touch. N. N
2. Vibration sense not felt on Lt lower limb but it slightly felt on rt lower limb
3. Position sense. N. N
4. Romberg’s sign - positive
III – CORTICAL
1. Two point
discrimination.
2. Tactile localisation. Not localised at some points and he delayed to localise the point at other regions in both lower limbs
3. Graphaesthesia. N. N
4. Stereognosis. N. N
Finger nose Coordination present
No dysdiadokinesia
Knee heel coordination present
Gait. Appear to be normal
Swaying seen when he walks on narrow path
And discomfort seen while walking down stairs
Provisional diagnosis
C5- C6 compressive MYELOPATHY
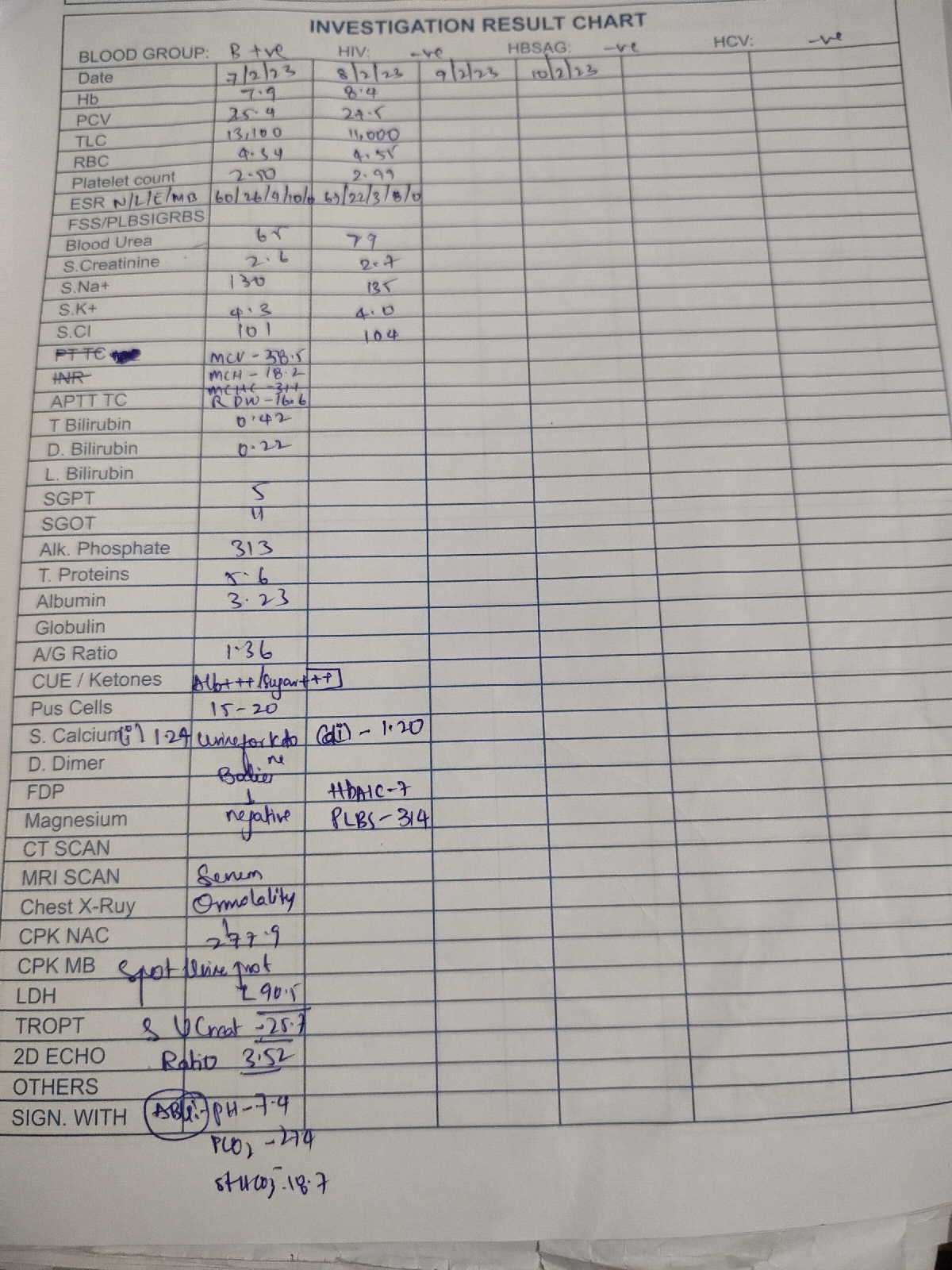
Investigation
Electrolytes
Na 139
K. 4.2
Cl. 104
Blood urea 26
S creatinine 0.9
RBS 95
FBS 87
Hba1c 6.5%
Hemogram
Hb 10.6
TLC 8200
PLT 2.27
CUE
Albumin and sugar nil
Serology
Negative
2d echo
EF 62%
TRIVIAL TR+,AR+ , No MR
No RWMA ,No As/MS
Good Lv systolic function
No diastolic dysfunction ,no pah.
Ecg
C3-C4,C4-C5,C6-C7 disc degeneration
C5-C6 disc osteophyte complex causing mederate cord compression with cord edema /early myelomalacia
Treatment
Pregabalin M 75po/hs
Definitive treatment
Pt need s anterior cervical decompression and fusion