40 yr old female presented in unresponsive state
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.


This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : SANTOSH KUMAR .K ( Intern )
Roll Number : 62
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
CHIEF COMPLAINTS
[27/12, 07:19] Patient came to casuality in unresponsive state since 4 pm in the evening, Blood pressure and Pulse rate are not recordable and SpO2 is 60%@RA and Central pulses are not felt, CPR was initiated and Patient was intubated mean while.
HOPI:
Patient was apparently asymptomatic 15 days ago, then she had sudden onset of severe headache, diffuse in nature, gradually progressive,which was present throughout the day, intensity of headache increased from 20/12/2022; for which she was sought for consultation at area hospital, CT Brain was done which showed old calcified granuloma and mild cerebral edema ( as documented by the area hospital physician). On 25/12/2022 around at 3 pm, patient has increased intensity of headache and lost consciousness and was unresponsive l, she was taken to local hospital and referred to our hospital.
[27/12, 07:42] PAST ILLNESS:
No Comorbidities
PERSONAL HISTORY:
Appetite normal.
Sleep inadequate
Bowel and Bladder regular.
No allergies.
No addictions.
GENERAL PHYSICAL EXAMINATION:
Patient
GCS : E1V1M1
No pallor, cyanosis, clubbing, lymphadenopathy, koilonychia,Icterus and Edema
VITALS
Temp 98.4°F; PR : not recordable; BP : Not recordable; RR: in gasping; SpO2 60%@RA; GRBS: 288 mg/dl.pupils fixed nd dilated. And non reactive to pupil
CVS : heart sounds not heard
R/S : Breath sounds not heard.
P/A :
Shape of abdomen: scaphoid.
Tenderness unable to elicit.
No palpable mass.
Hernial orifices normal.
Free fluid absent.
No bruits.
No organomegaly.
Bowel sounds absent.
CNS:
Level of consciousness: Coma
Speech: no response.
Cranial nerves: unable to elicit.
Motor system: Unable to elicit.
Sensory system: Unable to elicit.
Cerebellar signs: Unable to elicit.
POST CPR STATUS
PT IS INTUBATED
E1V1M1
BP. NR
HR 100BPM
CVS S1S2 HEARD
R/S BAE +
PUPILS. DILATED FIXED NON REACTIVE
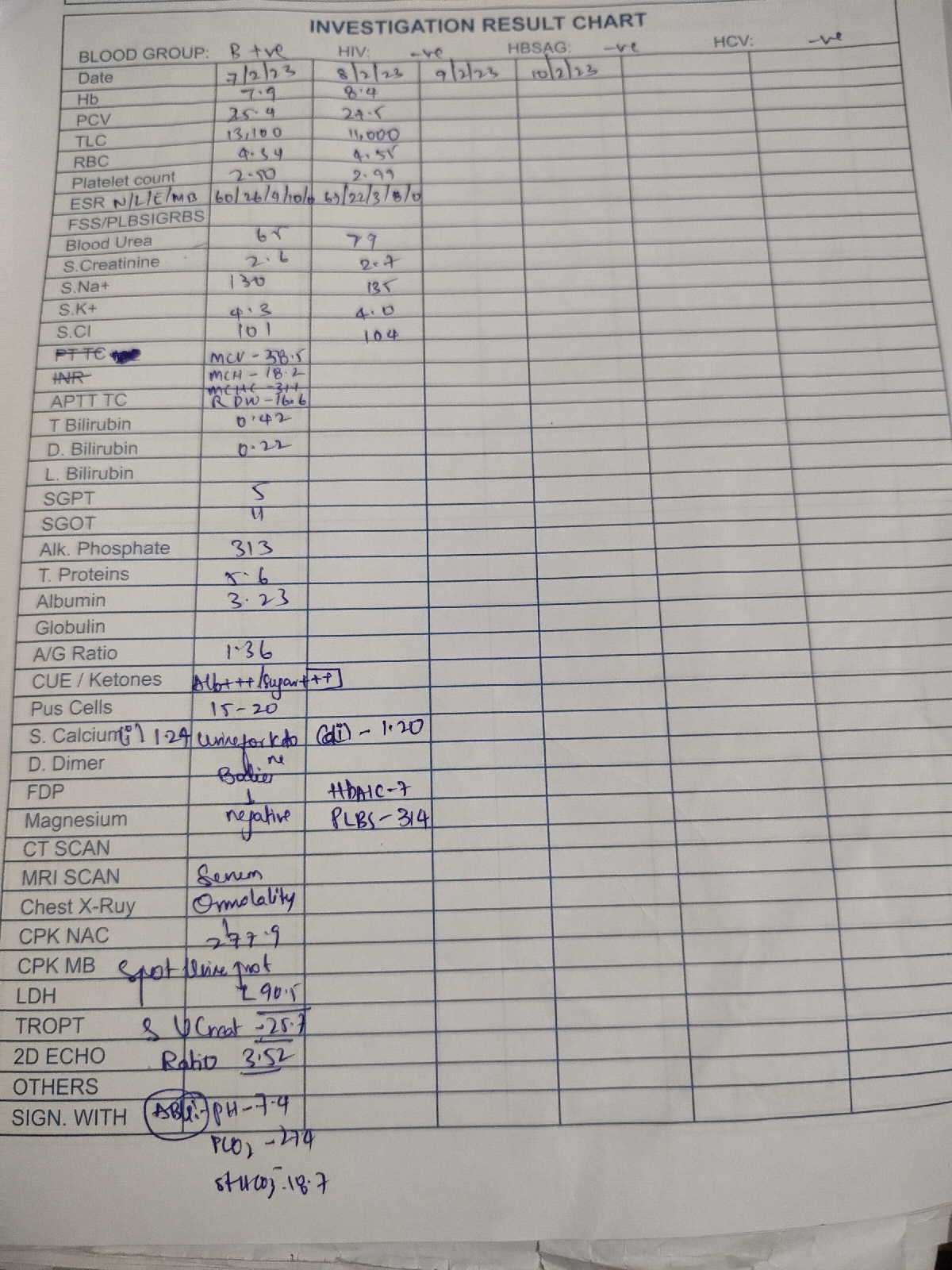
Investigation
2d Echo showed :
RWMA+; LAD Hypokinetic; RCA and LCx hypokinesia; Mild MR; Mild to Moderate TR with PAH; Eccentric TR; Trivial AR; No AS/MS; IAS Intact; EF 47%; Mild to Moderate LV Dysfunction; No diastolic dysfunction; minimal Pericardial Effusion; IVC size 1.66 cms- Mild dilated non collapsable; Mild dialted RA and RV.
PROVISIONAL DIAGNOSIS:
ALTERED SENSORIUM UNDER EVALUATION .
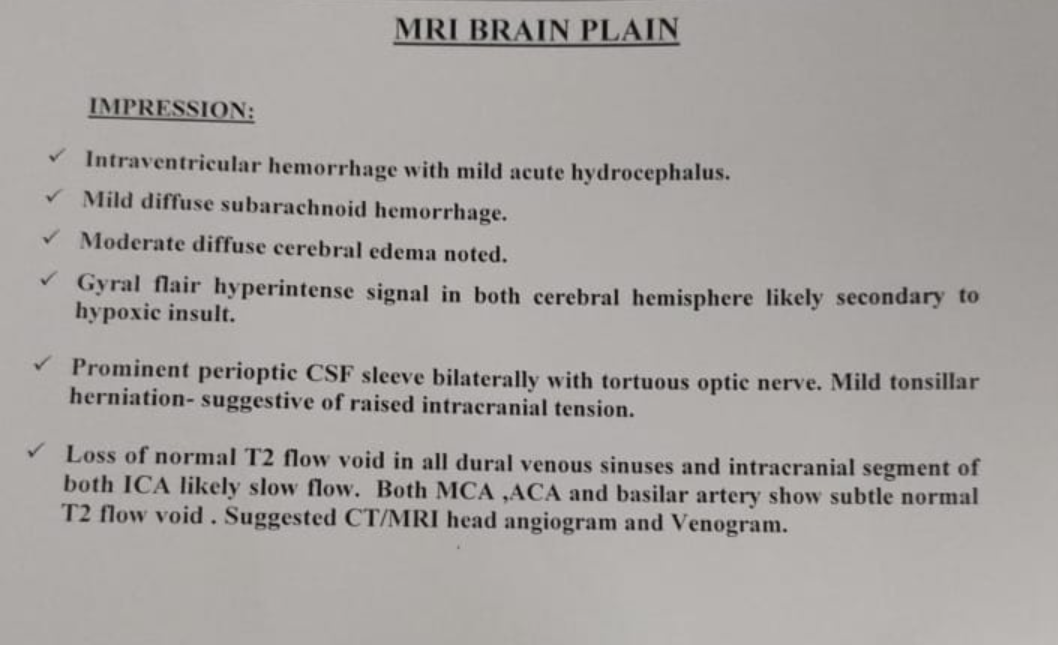
MRI report
Patient is on Mechanical Ventilation
Mode : ACMV- VC
PEEP: 5
Fio2 : 50 %
VT : 400ml
RR: 16 cpm.
Treatment
1. INJ. LEVIPIL 1 gr/IV/ STAT FOLLOWED BY INJ. LEVIPIL 500mg /IV / BD.
2. INJ. PIPTAZ 4.5 gram /IV / STAT FOLLOWED BY INJ. PIPTAZ 4.5 gram / IV / TID.
3. INJ. ZOFER 4 mg / IV / TID
4. INJ. NORADRENALINE (2 ampules in 46 ml NS ) increase or decrease according to MAP
5. INJ. DOBUTAMINE ( 1 Ampule in 45 ml NS) Increase or decrese according to MAP.
6. INJ. VASOPRESSIN
7. INJ. HYDROCORT 100 mg/IV / BD