I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
Following is the view of my case :
A 70-year-old male has presented to the hospital on 06 June 2022 with the chief complaints ofslurring of speech And difficulty in walking and weakness of right upper and lower limbs
It is from 9 days
Time line of events are :
HISTORY OF PRESENT ILLNESS:
. He
wake up every day at about 6am, freshen up, have breakfast and do his daily activities like grazing the cattle till the afternoon. He would then have lunch and take a nap till evening. He spend time with the neighbours for rest of the day.
Patient was apparently asymptomatic 3 yrs ago then he developed weakness of RT upper limb and lower limb which is sudden in onset which was treated and he recovered
Second episode of RT upper limb and lower limb weakness and dropping of mouth , drooling of saliva developed 1 year back. It was treated and he recovered
Third episode: He developed weakness of the right upper and lower limbs 9 days ago. He first was not able to walk then eat and then developed speech abnormality. Local doctor advised the patient to go to the hospital due to high blood pressure and symptoms are sudden in onset and progressed gradually.
Past history
- not a known case of diabetes, asthma, epilepsy, or TB.
- diagnosed with hypertension 10 months ago and has been using atenolol 25mg daily.
Personal history
DIET- mixed
Appetite: Normal
Bowel and bladder movements are regular
Sleep: Adequate
No known addictions and allergies.
General examination
General examination conscious , incoherent, cooperative
No pallor
Icterus
Cyanosis
Clubing
Lymphadenopathy
Vitals
BP 120/70mmhg
PR 79 BPM
RR 20
Spo2 95
Systemic examination
Respiratory examination
BAE +ve and normal vesicular breath sound heard
No crepts heard
CVS examination
S1S2 heard
No murmurs heard
Abdomen examination
Soft non tender
No hepatomegaly and splenomegaly
CNS:
Higher mental functions
conscious and cooperative but incoherent
oriented to time,
memory- not able to recognize family members but now able to recognise
Speech - Broca's aphasia ( only comprehension, no fluency, no repetition)
Cranial nerve examination:
I- Olfactory nerve- sense of smell present
II- Optic nerve- direct and indirect light reflex present
III- Oculomotor nerve, IV- Trochlear and VI- Abducens- normal eye movement no diplopia
V- Trigeminal nerve- sensory and motor function are intact
VII- Facial nerve- face is symmetrical, left nasolabial fold prominent than right. And drooling of saliva from RT side and unable to clench his teeth
VIII- Vestibulocochlear nerve- no hearing loss
IX- Glossopharyngeal nerve. X- Vagus- uvula not visualised
XI- Accessory nerve- sternocleidomastoid contraction present
XII- Hypoglossal nerve- Movements of tongue are normal, no fasciculations, no deviation of tongue
Sensory system examination:
Right Left
crude touch present present
fine touch absent present
pain. absent present
vibration absent present
temperature absent present
stereognosis- absent. present
2 pt discrimination-. absent present
graphaesthesia- absent present
Motor system examination
Right. Left
BULK: U/L- arm 24.5 cm 26 cm
-forearm 18 cm 18 cm
L/L- thigh 44 cm 44 cm
leg 28 cm 28 cm
Right Left
TONE: U/L decreased normal
L/L decreased normal
POWER: U/L- hand 0/5. 5/5
- elbow 2/5 4/5
- shoulder 0/5 5/5
L/L- hip 0/5 4/5
- knee 0/5 5/5
- ankle 0/5 4/5
Biceps. +++. ++
Triceps. +++. ++
Supinator. +++. ++
Knee. +++. ++
Ankle. +++. ++
COORDINATION: Absent
GAIT hemiplegic gait
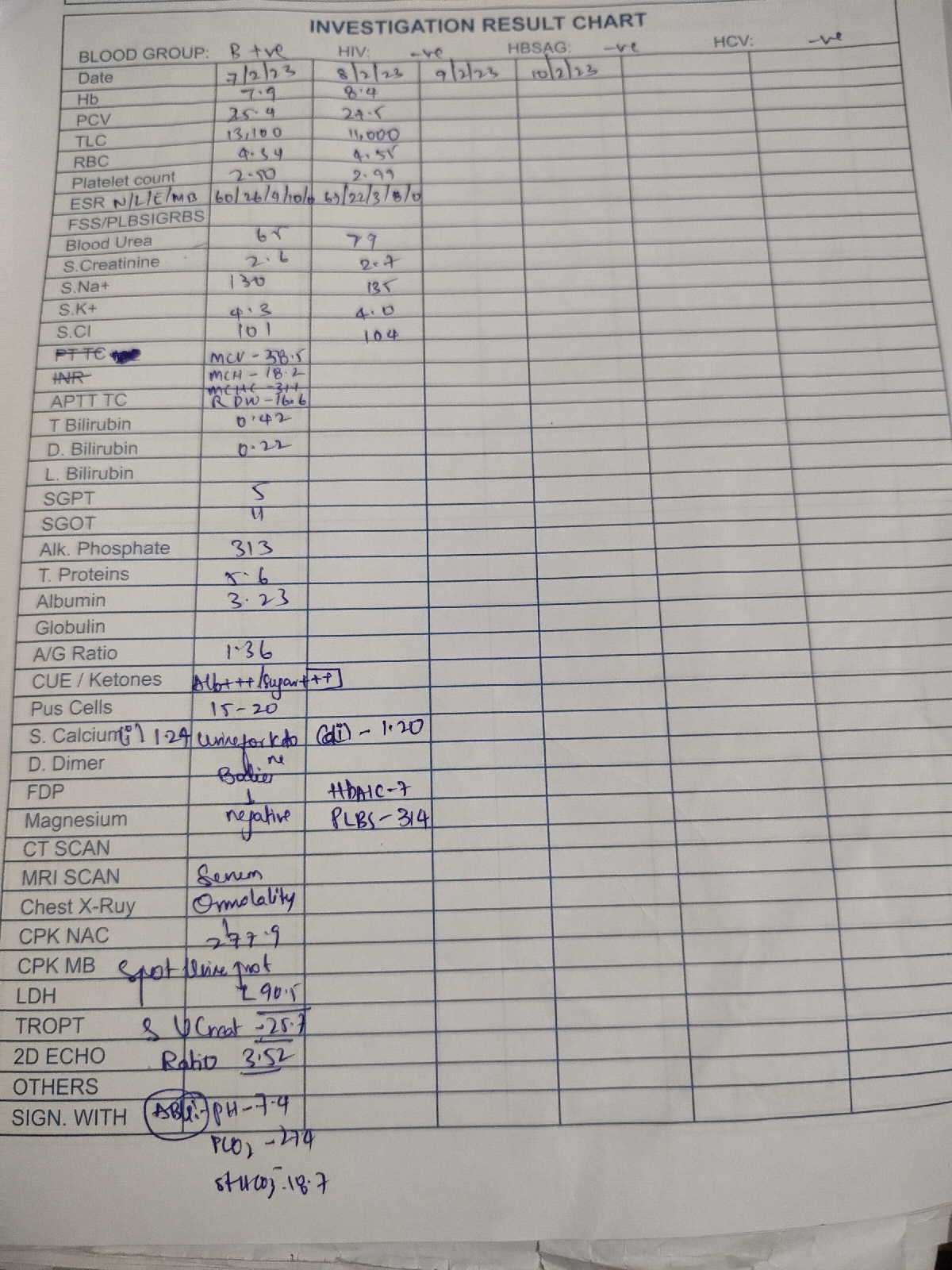
INVESTIGATIONS:
CBP
Hemoglobin- 12.6 gm/dl
PCV- 35.2 %
TLC- 8600/ cumm
RBC- 4.33 million/cumm
Platelets- 2.58 lakhs/ml
Blood urea- 24 mg/dl
Serum creatinine- 1.3 mg/dl
Serum sodium- 136 mEq/L
Serum potassium- 3.7 mmol/l
Serum chloride- 104 mEq/L
LFT
Total bilirubin- 0.61 mg/dl
Direct bilirubin- 0.16 mg/dl
SGPT- 11
SGOT- 13
ALP- 105 IU/L
Albumin- 4 g/dl
ECG
Carotid artery Doppler
Bilateral internal carotid artery stenosis Lt>Rt
PROVISIONAL DIAGNOSIS:
Acute ischemic stroke causing right sided hemiplegia (left MCA territory)
Recurrent CVA
TREATMENT:
Tab. Ecosporine 150mg
Tab. Clopidogrel 75 mg
Tab. Atorvas 40mg
Tab. Atenolol 25mg
Physiotherapy