Online Blended Bimonthly Assignment MAY 2021 Roll no. 52.
I have been given the following cases to solve in an attempt to understand the topic of 'patient clinical data analysis 'to develop my competency in reading and comprehending clinical data including history ,clinical findings, investigation and diagnosis and come up with the treatmentplan.
PULMONOLOGY
Case 1
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans)1st episode of sob - 20 yr back
2nd episode of sob - 12 yr back
From then she has been having yearly episodes for the past 12 yrs
Diagnosed with diabetis - 8yrs back
Anemia and took iron injections - 5yr ago
Generalised weakness - 1 month back
Diagnosed with hypertension - 20 days back
HRCT showed Signs of - 20 days ago
Bronchiectasis
Pedal edema - 15 days back
Facial puffiness- 15 days back
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans
Non pharmacoloical interventions .
1) oxygen inhalation - it is to maintain spo2
2)head end elevation. (Hobe)
improves oxygenation
.decreases incidence VAP
.decreases incidence of aspiration
Efficacy of Hobe
Significant increases in end-expiratory lung volume were seen at both 20° and 30° HOBE in all lung regions, except the anterior, with the largest changes from baseline (supine) seen at 30°. From baseline to 30° HOBE, global EELI increased by 1,327 impedance units (95% CI 1,080-1,573, P < .001).
Indications .
Brain trauma, bed ridden patients , hypoxic patients
3)Bipap:
Assist ventilation by delivering positive expiratory and inspiratory pressure with out need for Endotracheal intubation.
Efficacy of Bipap Over Placebo :
The 10 patients in the active NPPV group rapidly improved and none needed intubation. Placebo NPPV resulted in no change in the clinical condition of patients that continued to worsen and the 10 patients were crossed over to active NPPV. Three patients were intubated. No differences in terms of morbidity, length of stay or mortality between the two groups were observed. Active NPPV (but not placebo NPPV) led to a rapid and significant improvement in the clinical parameters, pH and the carbon dioxide tension in arterial blood and to a decrease in respiratory frequency and sternocleidomastoid EMG activity.
Pharmacological interventions
Drug therapy
1. Augmentin
It is a combination of Amoxicillin and clavulanic acid. Amoxicillin is a penicillin which is a cell wall synthesis inhibitor.
Penicillinase is an enzyme produced by the bacteria as a method of resistance to this antibiotic . Clavulanic acid inhibits the penicillinase thereby favouring the action of Amoxicillin
This is used to control spectrum.of bacterial infections.
2. Azithromycin
It is an antibiotic used to clear the bacterial infection in this patient which is thought to be the cause of Acute exacerbation of SOB in this patient
3. Lasix injection
It is a loop diuretic.
Acts by inhibiting Na k 2Cl channel
This patient has pedal edema which is upto ankle and is pitting type. Loop diuretics like furosemide are effective in control of pedal edema in this patient
4. Hydrocortisone
It is a steroid which os used to hasten the recovery in this patient. Enhancement in FEV1 and PaO2 in the patients with acute exacerbation of the COPD was achieved with steroids . This drug also reduce the duration in stay of hospital and also reduces tge rate of relapse at a later date.
5. Nebulization with bronchodilators
Budecort and Ipravent are the bronchodilators which are used to provide releif for acute attacks of dyspnea
6. Chest wall physiotherapy
It enhances the compliance of the chestwall and aids in recovery. It also strengthens the respiratory muscles.
7. GRBS charting
It is used to monitor glucose levels
8. Temperature BP and SPO2 monitoring
9. I/o charting
It is Indicated in hypertensive and diabetic patients
10.Thiamine
To prevent deficiency which may lead to neurological and cardiological deficits
3)what could be the causes for her current acute exacerbation
Ans)
- Acute bacterial infection
- Overlying heart problem as suggested by Echocardiogram
- Severe progression of disease.
- Allergic response to paddy dust
- Immunocompromised state as she is a diabetic and hypertensive
4) could the ATT have affect ed her symptoms?if so how?
Ans) NO
5) what could be the causes for her electrolyte imbalance?
Ans)Hyponatremia and hypochloremia might be due to the usage of Telmisartan as antihypertensive
NEUROLOGY
CASE - 02
https://143vibhahegde.blogspot.com/2021/05/wernickes-encephalopathy.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patiewernickes-encephalopath Evolution of symptomology;
detail 1 year ago-2 to 3 episodes of seizures
4 months ago-Following cessation of alcohol he developed seizures probably GTCS
9 days back-The patient started talking and laughing to himself
withdrawal seizures are triggered by neuronal networks in the brainstem, including the inferior colliculus.
Ethanol is the primary alcohol ingested by chronic users. It is a central nervous system (CNS) depressant that the body becomes reliant on with extended exposure to ethanol. It does this by inhibiting the excitatory portion (glutamate receptors) of the CNS and enhancing the inhibitory portions (GABA receptors) of the CNS. When the depressant is stopped, the central nervous system becomes overexcited as the inhibition is taken away. Thus, the body gets an excitatory overload, which results in the symptoms of withdrawal
Anatomical localisation:HIPPOCAMPUS AND FRONTAL LOBE
Prime etiology: CHRONIC ALCOHOLISM
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans)
as the aim of lowering the alcohol levels and its metabolites ,its neuro deppresive effects
and making patients spnding less in the ED
Thiamine
It helps the body cells change carbohydrates into energy.
It has been used as a supplement to cope with thiamine deficiency
Lorazepam
- binds to benzodiazepine receptors on the postsynaptic GABA-A ligand-gated chloride channel neuron at several sites within the central nervous system.
- it enhances the inhibitory effects of GABA, which increases the conductance of chloride ions into the cell
pregabalin
It reduces the synaptic release of several neurotransmitters, apparently by binding to alpha 2-delta sub-units, and possibly accounting for its actions invivo to reduce neuronal excitability and seizures.
Lactulose
It is used in preventing and treating clinical portal-systemic encephalopathy .its chief mechanism of action is by decreasing the intestinal production and absorption of ammonia.
Potchlor liquid is used to treat low levels of potassium in the body.
3) Why have neurological symptoms appeared this time, that were absent during withdrawal earlier? What could be a possible cause for this?
Ans)
Due to excess thiamine deficiency and excess toxins accumulation due to renal disease caused by excess alcohol addiction.
4) What is the reason for giving thiamine in this patient?
Ans) chronic alcohol cosumption causes thalamine deficiency due to impaired absorbstion of thalamine from the intestine A number of mechanisms may be involved in the pathogenesis of thiamin deficiency in the alcoholic population. An important cause is inadequate intake of thiamin. Moreover, there may be decreased conversation of thiamine to the active coenzyme, reduced hepatic storage of the vitamin in patients with fatty metamorphosis, ethanol inhibition of intestinal thiamine transport, and impaired thiamine absorption secondary to other states of nutritional deficiency
5) What is the probable reason for kidney injury in this patient?
Ans)The kidneys have an important job as a filter for harmful substances .alcohol causes changes in the function of the kidneys and makes them less able to filter the blood .alcohol also affects the ability to regulate fluid and electrolytes in the body. In addition, alcohol can disrupt hormones that disrupt hormones that affect kidney function .people who drink too much are more likely to have high blood pressure. High blood pressure is a common cause of kidney disease.
6). What is the probable cause for the normocytic anemia?
Ans)Anemia of chronic disease (ACD) is probably the most common type of anemia associated with COPD. ACD is driven by COPD-mediated systemic inflammation. Anemia in COPD is associated with greater healthcare resource utilization, impaired quality of life, decreased survival, and a greater likelihood of hospitalization. Anemia was normocytic and normochromic in nature. The exact cause of anemia of chronic disease may vary. Anemia can be caused by a slight shortening of normal red blood cell survival. the production of red blood cells (erythropoiesis) or erythropoietin (a hormone that stimulates red blood cell production) may be impaired.
7) Could chronic alcoholism have aggravated the foot ulcer formation? If yes, how and why?
Ans)Oxygen is important for cell metabolism and is critical for all wound-healing processes Inhibits wound healing by reducing the quantity and quality of oxygen to the wound site.
Case 3
https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans Timeline of the patient is as follows-
Patient was Diagnosed to Have DeNovo Hypertension in the Past But he did Not take any Medication.
7 days back- Patient gave a history of giddiness that started around 7 in the morning; subsided upon taking rest; associated with one episode of vomiting
4 days back- Patient consumed alcohol; He developed giddiness that was sudden onset, continuous and gradually progressive. It increased on standing and while walking.
H/O postural instability
Associated with bilateral hearing loss, aural fullness, presence of tinnitus
Associated vomiting- 2-3 episodes per day, non projectile, non bilious.
Present day of admission- Slurring of speech, deviation of mouth that got resolved the same day
Anatomical location- There is a presence of an infarct in the inferior cerebellar hemisphere of the brain.
Etiology-
Patient has hypertension for which he has been prescribed medication but he has not taken.There may be an Episode of Stroke which can be due to Ischemic or Heamorhagic cause resulting in reduced blood supply to the Cerebellar region resulting in Infarction.
2) What are the mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
ANS. The placebo has no physiological and pharmacological actions
1. Vertin
- It is an anti vertigo medicine.
- Composition: betahistine
- Indications:. Endolymphatic hydrops
- It is an H1 receptor agonist and H3 receptor antagonist
2.Zofer
- It is an anti-emetic
- It is a serotonin antagonist
3. Clopidogrel
It is an antiplatelet medication which is used in conditions such as impending stroke and in heart attack with aspirin
4. Atorvastatin
It is a HMG-coA reductase inhibitor which is used to lower blood cholesterol
5. Aspirin
It is a NSAID which works by inhibiting cyclooxygenase.
It is used in people with heart diseases and in management of heart attack
Most dangerous and rare side effect is Reyes syndrome
6. Multivitamin tablets
These are used to prevent vitamin deficits and also help to replenish the stores of fat soluble vitamins
Mvt Methylcobalamin is employed in cyanocobalamin deficiency.
Methylcobalamin could be a kind of vitamin B that restores its level within the body thereby helping in treating certain anemias and nerve problems
Methylcobalamin could be a kind of vitamin B that restores its level within the body thereby helping in treating certain anemias and nerve problems
3) Did the patients history of denovo HTN contribute to his current condition?
Ans Considering the history and fact that hypertension is a risk factor for CVAwe may presume that he might be a chronic hypertensive which was undiagnosed.
Smoking and alcohol history would add weight to this presumption as they are thought to be the risk factors for hypertension.
Alcohol is an independent risk factor for stroke.
4) Does the patients history of alcoholism make him more susceptible to ischaemic or haemorrhagic type of stroke?
Ans Yes, Atrial fibrillation and alcohol Drinking excessive amounts of alcohol can trigger atrial fibrillation – a type of irregulaR heartbeat. Atrial fibrillation increases your risk of stroke by five times, because it can cause blood clots to form in the heart. If these clots move up into the brain, it can lead to stroke.
Case 4
http://bejugamomnivasguptha.blogspot.com/2021/05/a-45-years-old-female-patient-with.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans
The patient has palpitations,pedal edema ,chest pain and heaviness , dragging type of pain in left upper limb all suggestive of a heart pathology
Previous history of hypokalemic paralysis suggestive of recurrent hypokalemic episodes
This might lead to auto compensation by kidney leading to reabsorption if the potassium along with water which might lead to pedal edema
Further the hypokalemia is known to cause physiological heart defects and ECG changes which could Be the cause for palpitations and left upper limbs paralysis
2) What are the reasons for recurrence of hypokalemia in her? Important risk factors for her hypokalemia?
Ans Important Risk factors for Hypokalemia :
1)Medications-diuretics, laxatives, enema.
2)alkalosis, 3)thyrotoxicosis,
4)anorexia, 5)dementia
Might be due to the usage of steroids from 8 months for relief from edema.
Recently it has been reported that the beneficial effect of steroids might be attributed to inhibition of edema spread or acceleration of edema resorption
3) What are the changes seen in ECG in case of hypokalemia and associated symptoms?
Ans ECG changes include flattening and inversion of T waves in mild hypokalemia, followed by Q-T interval prolongation, visible U wave and mild ST depression4 in more severe hypokalemia. Severe hypokalemia can also result in arrhythmias such as Torsades de points and ventricular tachycardia.
Case5
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
1. Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
Ans If you’ve had a stroke, you have an increased risk for having a seizure. A stroke causes your brain to become injured. The injury to your brain results in the formation of scar tissue, which affects the electrical activity in your brain. Disrupting the electrical activity can cause you to have a seizure.
2. In the previous episodes of seizures, patient didn't loose his consciousness but in the recent episode he lost his consciousness what might be the reason?
Ans. Abnormal increased activity in fronto-parietal association cortex and related subcortical structures is associated with loss of consciousness in generalized seizures. Abnormal decreased activity in these same networks may cause loss of conscious-ness in complex partial seizures. Thus, abnormally increased or decreased activity in the same networks can cause loss of consciousness. Information flow during normal conscious processing may require a dynamic balance between these two extremes of excitation and inhibition.
Case 6
https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
1) What could have been the reason for this patient to develop ataxia in the past 1 year?
Ans. By the history, Patient is an alcoholic and he has change in his gait since a year are the findings which leads to cause of ataxia.
Mechanism:Damage from alcohol is a common cause ofcerebellar ataxia. In patients with alcohol related ataxia, the symptoms affect gait (walking) and lower limbs more than arms and speech. It can also cause associated signs of peripheral neuropathy. Peripheral neuropathy is damage to the body's peripheral nervous system.
2) What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
Ans. Patient has a history of binge drinking for 3 hours before the day of admission.
Heavy drinkers were about 1.6 times more likely to suffer from intracerebral hemorrhage and 1.8 times more likely to suffer from subarachnoid hemorrhage. The association between heavy alcohol consumption and these two types of stroke was stronger than that for ischemic stroke. Yes alchol could have increased IC bleeding.Liver damage due to too much alcohol can stop the liver from making substances that help your blood to clot. This can increase your risk of having a stroke caused by bleeding in your brain.
Case7
http://shivanireddymedicalcasediscussion.blogspot.com/2021/05/a-30-yr-old-male-patient-with-weakness.html
1.Does the patient's history of road traffic accident have any role in his present condition?
Ans. One cause of stroke after trauma is a tear in the head or neck blood vessels that lead to the brain, which can be a source of blood clots that cause a stroke. If a tear in these arteries can be diagnosed at the time of the trauma, a patient could be treated with an anti-clotting medicine to help prevent stroke
2).What are warning signs of CVA??
Ans
Sudden NUMBNESS or weakness of face, arm, or leg, especially on one side of the body.
- Sudden CONFUSION, trouble speaking or understanding speech.
- Sudden TROUBLE SEEING in one or both eyes.
- Sudden TROUBLE WALKING, dizziness, loss of balance or coordination.
- Sudden SEVERE HEADACHE with no known cause.
3)What is the Drug rationale in CVA??
Ans Mannitol- Because of its osmotic effect, mannitol is assumed to decrease cerebral edema. Mannitol might improve cerebral perfusion by decreasing viscosity, and as a free-radical scavenger, it might act as a neuroprotectant.
Ecospirin
For the prevention of heart attack, stroke, heart conditions such as stable or unstable angina (chest pain) due to a blood clot.
Atrovas-Atorva 40 Tablet belongs to a group of medicines called statins. It is used to lower cholesterol and to reduce the risk of heart diseases. Cholesterol is a fatty substance that builds up in your blood vessels and causes narrowing, which may lead to a heart attack or stroke.
Rt feed RT feed is a nursing procedure to provide nutrition to those people who are either unable to obtain nutrition by mouth or are not in a state to swallow the food safely.

4)Does alcohol has any role in his attack?
AnsAs the patient is a chronic alcoholic, it is possible that alcohol migh have not played role in his attack
When the patient met with an accident there might be cranial damage which was unnoticed.
If so his occasional drinking may or may not have hindered the process of the minor hemorrhages getting healed and might have caused this condition
But since the patient is not a chronic alcoholic and so Alcohol might not have played any role.Therefore it cannot be evaluated without further details
5.Does his lipid profile has any role for his attack??
Yes increased LDL causes atherosclerosis which ultimately results in stroke.
Case 8
https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
1) What is myelopathy hand ??
Ans Loss of power of adduction and extension of the ulnar two or three fingers and an inability to grip and rapidly release with these fingers is termed as myelopathy hand. This is due to Pyramidal Tract Involvement.

Ans All patients exhibited myelopathy hand, which was defined by two specific signs: the finger escape sign and the inability to grip and release rapidly with the fingers. Fourteen 3-mm micro-reflective markers were placed on the dorsal surface of the thumb and the index finger, and on the dorsal hand.
- It is also called as WARTENBERG sign
3)What is Hoffman’s reflex?
Ans Hoffmanns reflex
When The investigator flicks the fingernail of middle finger down , there is an involuntary Flexion of thumb or index finger
This is called as positive Hoffman's reflex
It is seen in UMN lesions and corticospinal tract lesions
Case 9
https://neerajareddysingur.blogspot.com/2021/05/general-medicine-case-discussion.html?m=1
1) What can be the cause of her condition ?
Presence of Cortical Vein Thrombosis in Right Posterior Temporal Lobe.
2 ) What are the risk factors for cortical vein thrombosis?
Iron Deficiency Anemia
Hereditary Thrombophilia
Trauma
Sickle Cell Anemia
4) What drug was used in suspicion of cortical venous sinus thrombosis ??
Clexane - Enoxaparin was used in Suspicion of Cortical Venous Sinus Thrombosis
3) There was seizure free period in between but again sudden episode of GTCS why?resolved spontaneously why?
ANSWER
The postictal state is the altered state of consciousness after an epileptic seizure. It usually lasts between 5 and 30 minutes, but sometimes longer in the case of larger or more severe seizures, and is characterised by drowsiness, confusion, nausea, hypertension, headache or migraine, and other disorienting symptoms
CARDIOLOGY
Case 10
https://muskaangoyal.blogspot.com/2021/05/a-78year-old-male-with-shortness-of.html.
1).What is the difference btw heart failure with preserved ejection fraction and with reduced ejection fraction?
Ans
Despite the fact that HFrEF and HFpEF share many risk factors and co-morbidities, there are substantial differences in systemic inflammation, cardiac remodelling (endothelial function, hypertrophy, and cardiomyocyte cell death), and stiffness (fibrosis, titin, and calcium levels). HFrEF, mostly occurs in male patients and is the consequence of cardiomyocyte loss. In contrast, HFpEF is often diagnosed in elderly female patients, who suffer from (a cluster of) non-cardiac comorbidities, such as hypertension, T2DM, stroke, anaemia, pulmonary disease, liver disease, sleep apnoea, gout, and cancer. HFpEF is characterized by low-grade chronic systemic inflammation and capillary dysfunction, with consequential low-grade cardiac inflammation. However, as most studies are conducted on models of established HFpEF, studies during the disease onset are required to elucidate the common denominator underlying the associated complications for HFpEF. In HFrEF, systemic and cardiac inflammation are secondary to the causes of cardiomyocyte loss. Whereas in HFpEF endothelial dysfunction mainly precedes its progression, in HFrEF endothelial dysfunction may rather be the consequence. Depending on the stimulus, perivascular (metabolic risks in HFpEF), interstitial (e.g., aging, hypertension in both HFpEF and HFrEF), or replacement (e.g., MI in HFrEF) fibrosis occurs and is differentially managed between the two conditions. The increased left ventricular stiffness in HFpEF is caused by reduced Ca2+ signalling, titin modifications (isoform shifts towards the stiffer isoform and post-translational changes), and increased perivascular and interstitial fibrosis. In contrast, in HFrEF, titin isoform switching is less consistent, and more flexible isoforms even present in end-stage non-ischemic dilated cardiomyopathy, therefore left ventricular stiffness ranges from being unaffected, to increased, or even reduced.
2.Why haven't we done pericardiocenetis in this pateint?
Ans
As the condition is resolving, there is not need for pericardiocentesis
3.What are the risk factors for development of heart failure in the patient?
Ans
- hypertension
- CAD
- DM
- MEDICATIONS
4.What could be the cause for hypotension in this patient?
Ans
THE VENOUS RETURN IN THIS PATIENT IS LOW ,WHICH IN TURN LEADS TO LOW CARDIAC OUTPUT THEREBY LEADING TO HYPOTENSION
Case 11
https://muskaangoyal.blogspot.com/2021/05/a-73-year-old-male-patient-with-pedal.html
1.What are the possible causes for heart failure in this patient?
Ans
Alcoholic cardiomyopathy is a form of heart disease caused by alcohol abuse. Long-term alcohol abuse weakens and thins the heart muscle, affecting its ability to pump blood
high blood glucose from diabetes can damage your blood vessels and the nerves that control your heart and blood vessels
High blood pressure can strain your heart, damage blood vessels, and increase your risk of heart attack
Diseases in the kidneys can affect the heart. It is common for people with chronic kidney disease or end-stage kidney disease to develop heart disease, including heart attack or heart failure.
2.what is the reason for anaemia in this case?
Ans
When you have kidney disease, your kidneys cannot make enough EPO. Low EPO levels cause your red blood cell count to drop and anemia to develop. Most people with kidney disease will develop anemia. Anemia can happen early in the course of kidney disease and grow worse as kidneys fail and can no longer make EPO
3.What is the reason for blebs and non healing ulcer in the legs of this patient?
Ans
Diabetes mellitus
4. What sequence of stages of diabetes has been noted in this patient?
Ans:stage 1: defined as DCBD (dysglycemia-based chronic disease )insulin resistance;
stage 2: defined as DCBD prediabetes;
stage 3: defined as DCBD type 2 diabetes; and
stage 4: defined as DCBD vascular complications, including retinopathy, nephropathy or neuropathy, and/or type 2 diabetes-related microvascular events.
All these stages have been noted in this case
Case 12
https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
1)What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?Ans Shortness of Breath - From 2 DAYS.
Decreased Urine Output-From 2 Days
Anatomical Localization : Heart
Etiology : Atrial Fibrillation
2)What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans. Inj.Dobutamine -Ionotropic Action so Increase the force of. Contraction
Tab.Digoxin - Ionotropic Effect
Diuretics Are also used
Beta Blockers is also used.
3) What is the pathogenesis of renal involvement due to heart failure (cardio renal syndrome)? Which type of cardio renal syndrome is this patient?
Cardiorenal syndromes (CRS) describe concomitant bidirectional dysfunction of the heart and kidneys in which 1 organ initiates, perpetuates, and/or accelerates decline of the other. CRS are common in heart failure.

4) What are the risk factors for atherosclerosis in this patient?
Ans
High cholesterol and triglyceride levels.
High blood pressure.
Smoking.
Type 1 diabetes.
Obesity.
Physical inactivity.
High saturated fat diet.t?
5) Why was the patient asked to get those APTT, INR tests for review?
Ans
Standard coagulation screening tests such as activated partial thromboplastin time (APTT), prothrombin time (PT), and the international normalized ratio (INR) are important constituents of basic examinations in clinical laboratories. APTT can be used as an indicator of intrinsic coagulation pathway activity, and a short APTT is linked to increased thrombin generation and increased risk for thrombosis.
Case 13
https://daddalavineeshachowdary.blogspot.com/2021/05/67-year-old-patient-with-acute-coronary.html?m=1
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
TIMELINE OF EVENTS-
• Diabetes since 12 years - on medication
• Heart burn like episodes since an year- relieved without medication
• Diagnosed with pulmonary TB 7 months ago- completed full course of treatment, presently sputum negative.
• Hypertension since 6 months - on medication
• Patient presented with Shortness of Breath
Anatomical localisation - Cardiovascular system
Etiology: The patient is both Hypertensive and diabetic and these may result in the development of atherosclerosis.
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Pharmacological interventions:
TAB MET XL 25 MG/STAT-contains Metoprolol as active ingredient
MOA: METOPROLOL is a cardiselective beta blocker
Beta blockers work by blocking the effects of the hormone epinephrine. Beta blockers have a negative chronotropic effect
and negative inotropic effect.
Beta blockers also have antiarrhythmic effects and also anti ischemic effects. They also inhibit renin.
EFFICACY STUDIES.
In CAD, 12 meta-analyses (93 RCTs, 103,481 patients) showed that beta-blockers reduced mortality in analyses before routine reperfusion, but there was a lack of benefit in contemporary studies where ≥ 50% of patients received thrombolytics or intervention.
Non pharmacological intervention advised to this patient is: PERCUTANEOUS CORONARY INTERVENTION.
Percutaneous Coronary Intervention is a non-surgical procedure that uses a catheter (a thin flexible tube) to place a small structure called a stent to open up blood vessels in the heart that have been narrowed by plaque buildup ( atherosclerosis).

3) What are the indications and contraindications for PCI?
INDICATIONS:

CONTRAINDICATIONS:
Absence of cardiac surgery backup.
Hypercoagulable state.
High-grade chronic kidney disease.
Chronic total occlusion of SVG.
4) What happens if a PCI is performed in a patient who does not need it? What are the harms of overtreatment and why is research on overtesting and overtreatment important to current healthcare systems?
Although PCI is generally a safe procedure , it might cause serious certain complications like
A)Bleeding
B) Blood vessel damage
C) Allergic reaction to the contrast dye used
D) Arrhythmias
E) Need for emergency coronary artery bypass grafting .
⁃ OVER TESTING AND OVER TREATMENT :
In olden days doctors would so much depend on their intuition as technology was not available .But these days every physician is dependent on laboratory reports.We cannot say it is a bad thing as it would lead to accurate diagnosis, but the point is these should be used logically only where they are required.Or else it would lead to overtesting.And overtesting has its own adverse effects.For example during the recent 2nd wave of Covid Pandemic majority of the Covid Patients including the asymptomatic and patients with mild disease were advised to take CT Scan which lead to unwanted radiation exposure.Even overtreatment has its own adverse effects.So even though all the Therapeutic and Diagnostic Facilities are available at our disposal , Physicians should use them Judiciously or Else they will do more harm than good.
Case 14
https://bhavaniv.blogspot.com/2021/05/case-discussion-on-myocardial-infarction.html?m=1
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans
Evolution of symptomatology:
Uncontrolled DM2 since 8 years
3 days back Mild chest pain dragging type and retrosternal pain(radiated)
Anatomical localisation: Inferior wall of heart
Primary etiology: Diabetes type 2 (uncontrolled)
high blood glucose from diabetes can damage your blood vessels and the nerves that control your heart and blood vessels
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans
TAB. ASPIRIN 325 mg PO/STAT
Mechanism of action: The acetyl group of acetylsalicylic acid binds with a serine residue of the cyclooxygenase-1 (COX-1) enzyme, leading to irreversible inhibition. This prevents the production of pain-causing prostaglandins.
TAB ATORVAS 80mg PO/STAT
Mechanism of action: Atorvastatin competitively inhibits 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase. By preventing the conversion of HMG-CoA to mevalonate, statin medications decrease cholesterol production in the liver.
TAB CLOPIBB 300mg PO/STAT
Mechanism of action: The active metabolite of clopidogrelselectively inhibits the binding of adenosine diphosphate (ADP) to its platelet P2Y12 receptor and the subsequent ADP- mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting platelet aggregation. This action is irreversible.
INJ HAI 6U/IV STAT
VITAL MONITORING.
3) Did the secondary PTCA do any good to the patient or was it unnecessary?
Ans:
Repeat PTCA provides a valuable, safe and cost-effective way of management for recurrence of stenosis after initially successful angioplasty. It increased the percent of patients with documented long-term success of angioplasty
Over testing and over treatment can raise a person’s risk of cardiovascular death by as much as four times.
Case 15
https://kattekolasathwik.blogspot.com/2021/05/a-case-of-cardiogenic-shock.h
1. How did the patient get relieved from his shortness of breath after i.v fluids administration by rural medical practitioner?
AnsFluids and plasma are given through an IV. Medications to treat cardiogenic shock are given to increase your heart's pumping ability and reduce the risk of blood clots.
2. What is the rationale of using torsemide in this patient?
Ans Torsemide is an antihypertensive diuretic causes decrease in blood pressure, here patient is already hypotensive, then what is the need to give this torsemide and decrease the BP further?
3. Was the rationale for administration of ceftriaxone? Was it prophylactic or for the treatment of UTI?
Ansl: There was whitish discharge in the Urine.Hence patient was given Ceftriaxone to treat UTI.
GASTROENTEROLOGY
Case 16
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-pancreatitis-with.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans
Evolution of symptomatology and event timeline -
- Pain abdomen and vomiting ; was treated conservatively 5 YRS AGO
- Pain abdomen and vomiting Since 1 week
- Constipation, burning micturition, fever Since 4 days
After admission -
- CT scan - showed pseudocyst
- Chest X ray - showed left pneumothorax and left pleural effusion
Primary etiology - Chronic alcohol intake
2) What is the efficacy of drugs used along with other non pharmacological treatment modalities and how would you approach this patient as a treating physician?
Ans
Amikacin, metronidazole and meropenamare all.given to control infection.
TPN : total parenteral nutrition
It is given to bed ridden patients.it contains carbohydrates,proteins, fats vitamins and minerals
NS/RL
It is given as fluid replacement inorder to combat dehydration
Tab.Pantop
It is a proton pump inhibitor.it is used in this case for its anti pancreatic secretory
Inj.octreotide
It is a somatostatin analogue
It decreases the secretions of pancreas
It also has anti inflammatory and cytoprotective effects
Inj.Thiamine
It is B1 supplement.
It is given here because; due to long fasting & TPN usage , body may develop B1 deficiency
Wernicke encephalopathy secondary to B1 deficiency may be caused... so a prophylactic B1 supplemention is necessary.
Inj.TRAMADOL
It is an opioid analgesic which is given to relieve pain.
Case 17
https://nehae-logs.blogspot.com/2021/05/case-discussion-on-25-year-old-male.html
1) What is causing the patient's dyspnea? How is it related to pancreatitis?
May be Pancreatitis is the Cause of Patients Dyspnea.Once Pancreatitis is initiated the inflammatory events within the acinar cells will progress to a generalized systemic inflammatory response syndrome (SIRS). Amongst the systemic complications, pulmonary complications are the most frequent and potentially the most serious.
The most dangerous complication of the pulmonary system is ARDS.
Activated trypsin causes damage to pulmonary vasculature and increases endothelial permeability. Active circulating phospholipase A2 (PLA2) is known to remove fatty acids from phospholipids. One of the main components of surfactant is the phospholipid, dipalmitoylphosphatidylcholine. Many recent studies have assessed the role of platelet activating factor (PAF) which stimulates polymorphonuclear cells (PMNs) regulating the interaction between PMNs and endothelial cells facilitating migration of activated WBC into interstitial spaces.
There are pro-inflammatory cytokines released from the pancreas such as tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1, IL-6, and IL-8. PMNs also contribute to release of cytokines
https://www.pulmonologyadvisor.com/home/decision-support-in-medicine/pulmonary-medicine/pulmonary-complications-of-liver-disease/#:~:text=Ascites%20elevates%20the%20diaphragms%20and,pleural%20effusion%20termed%20a%20hydrothorax
2) Name possible reasons why the patient has developed a state of hyperglycemia.
Ans
Pancreatitis results in damage to beta cells. Results in decreased insulin and hyperglycemia
This hyperglycemia could thus be the result of a hyperglucagonemia secondary to stress or the result of decreased synthesis and release of insulin secondary to the damage of pancreatic β-cells
3) What is the reason for his elevated LFTs? Is there a specific marker for Alcoholic Fatty Liver disease?
Ans
The most common causes of acute pancreatitis are gallstones and alcohol-induced pancreatitis. This patientss liver enzymes (especially ALT) and bilirubin level are elevated, which may suggest choledo- cholithiasis.
The biochemical markers of a biliary etiology of acute pancreatitis (AP) include an ALT elevation of more than 3 times the upper range of normal (ULN) and a serum total bilirubin greater than 3 mg%
4) What is the line of treatment in this patient?
Ans
iv fluids and colloids
NPO (Nill Per Oral)
Analgesics
Nasogastric suction -to decrease gastrin release from stomach
laparotomy and debridement of hemorrhagic pancreatic tissue.
antibiotic therapy like ciprofloxacin , ofloxacin, imipenem
Case18
https://chennabhavana.blogspot.com/2021/05/general-medicine-case-discussion-1.html
1) what is the most probable diagnosis in this patient?
AnsAbdominal Hemorrhage may be the most probable diagnosis in this patient.
2) What was the cause of her death?
Ans:Cause of her death may be due to complications of laparotomy surgery such as hemorrhage, infection, or damage to internl organs.
3) Does her NSAID abuse have something to do with her condition? How?
Ans:NSAIDS are known to cause drug induced hepatitis which may lead to cirrhosis.
NSAID inhibit the synthesis of prostaglandins. prostaglandins are required for the direction of the afferent arteriole of the kidney. But as their synthesis is inhibited there will be no afferent arteriolar dilation and reduced glomerular perfusion this may lead to pre renal acute kidney injury.Chronic NSAIDs use has also been related to hepatotoxicity. While the other adverse effects of NSAIDs such as are well known, gastrointestinal mucosal injury NSAIDs have also been associated with hepatic side effects ranging from asymptomatic elevations in serum aminotransferase levels and hepatitis with jaundice to fulminant liver failure and death.
NEPHROLOGY
Case19
https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html
1) What could be the reason for SOB??
As the patient was administered diuretics may be it has lead to increased excretion of Bicarbonate ions.So there will be Metabolic Acidosis.To compensate that there will be increase in the respiratory rate to eliminate the CO2 so that equilibrium is maintained.Hence there will be Shortness of Breath due to increased respiratory rate.
2) Why does he have intermittent episodes of drowsiness??
Use of Diuretics has lead to Hyponatremia which resulted in Drowsiness.
3)Why did he complain of fleshy mass like passage in urine ??
There are large no. Of puss cells in his urine.May be the patient confused these with a fleshy Mass.
4)What are the complications of TURP that he may have had ??
TURP -Transurethral resection of Prostate
- May be Glycerol used for bladder wash during the procedure has caused some damage to the kidney.There was a rise in his creatinine levels following the procedure.
There is also chance of infection.
Patient's WBC count is also Raised.
Case 20
https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.html
1.)Why is the child excessively hyperactive without much of social etiquettes
Ans
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by inattention, or excessive activity and impulsivity, which are otherwise not appropriate for a person's age
For a diagnosis, the symptoms have to be present for more than six months, and cause problems in at least two settings (such as school, home, work, or recreational activities).
2.) Why doesn't the child have the excessive urge of urination at night time ?
Ans
Since the child doesn’t have excessive urge of urination at night but at day there might be a psychiatry related condition
1. Psychosomatic disorder
2. Undiagnosed anxiety disorder
3.)How would you want to manage the patient to relieve him of his symptoms?
Ans
bacterial kidney infection, the typical course of treatment is antibiotic and painkiller therapy.
If the cause is an overactive bladder, a medication known as an anticholinergic may be used. These prevent abnormal involuntary detrusor muscle contractions from occurring in the wall of the bladder
INFECTIOUS DISEASES
Case21
https://vyshnavikonakalla.blogspot.com/2021/05/a-40-year-old-lady-with-dysphagia-fever.html
1)Which clinical history and physical findings are characteristic of tracheo esophageal fistula?
Laryngeal Crepitus,Difficulty in swallowing initially to the solids,
Cough,are Suggestive of TracheoEsophageal Fistula.
2)What are the chances of this patient developing immune reconstitution inflammatory syndrome? Can we prevent it?
Risk Factors For Development of Immune Reconstitution Inflammatory Syndrome (IRIS)
1) Low Baseline CD4 Count
2) Higher Baseline Viral Load
3) Shorter Interval between commencing ATT and HAART
4) Disseminated TB
5) A Greater Decrease in Viral Load after starting HAART.
As this patient has a low baseline CD4 count and also disseminated TB there are chances that this patient may develop IRIS.

Case 22
https://kavyasamudrala.blogspot.com/2021/05/liver-abscess.html
1. Do you think drinking locally made alcohol caused liver abscess in this patient due to predisposing factors present in it ? What could be the cause in this patient ?
Ans
it was undoubtedly proved that alcoholism, mainly consuming locally prepared alcohol plays a major role as a predisposing factor for the formation of liver abscesses that is both amoebic as well as pyogenic liver abscess because of the adverse effects of alcohol over the Liver. It is also proven that Alcoholism is never an etiological factor for the formation of liver abscess.
2. What is the etiopathogenesis of liver abscess in a chronic alcoholic patient ? ( since 30 years - 1 bottle per day
Ans
Alcohol changes gut permeability, increasing absorption of endotoxins released by bacteria in the gut. In response to the endotoxins (which the impaired liver can no longer detoxify), liver macrophages (Kupffer cells) release free radicals, increasing oxidative damage.
3. Is liver abscess more common right lobe
Ans
50% of solitary liver abscesses occur in the right lobe of the liver (a more significant part with more blood supply), less commonly in the left liver lobe or caudate lobe
4.What are the indications for ultrasound guided aspiration of liver abscess ?
Ans
Ultrasound guided percutaneous drainage is one form of image guided procedure, allowing minimally invasive treatment of collections that are accessible by ultrasound study.
Indications for percutaneous drainage are broad: essentially any abnormal fluid collection in the patient which can be accessible. Examples include:
complicated diverticular abscess
Crohn's disease related abscess
complicated appendicitis with appendicular abscess
tuboovarian abscess
post-surgical fluid collections
hepatic abscess (e.g. amoebic or post-operative)
renal abscess or retroperitoneal abscess
splenic abscess
Case 23
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
1) Cause of liver Abcess in this Patient??
May be due to malnutrition and lack ofpersonal hygeine is the cause of the infection in the patient resulting in liver abcess. The infection may be amoebic or any other bacterial infection.
2) How do you approach this Patient??
As the patient presented with the pain in the abdomen, first I would go for a USG abdomen and As USG showing hyperechoic mass on the liver I would also do LFT(Liverfunction Test)
As there is a mass as seen in USG and LFT is also abnormal (Raised ALP), I would start empirical Treatment for both Amoebic and pyogenic liver abscess.
According to the response given to this Medical Treatment it will be decided whether aspiration is required or not.

3) Why do we treat here ; both amoebic and pyogenic liver abcess?
Ans: to prevent the secondary bacterial infections in amoebic liver abscess and also we cannot take risk until we confirm it as amoebic
Hence we need to administer antibiotics too
4) Is there a way to confirm the definitive diagnosis in this patient?
Ans
Ultrasound abdomen followed by CT scan and blood tests
Amoebic specific tests
Case 24
http://manikaraovinay.blogspot.com/2021/05/50male-came-in-altered-sensorium.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem
Ans
Patient is a known hypertensive from past 3 years.
He went for covid 19 vaccination and from that night he's complaining of fever with chills and rigor.
Facial puffiness amd periorbital edema after 10 days of vaccination
Theb afterwards he developed weakness in right upper amd lower limb.
Then after one week , he presented with altered sensorium
2) What is the efficacy of drugs used along with other non pharmacological treatment modalities and how would you approach this patient as a treating physician?
Ans
LIPOSOMAL AMPHOTERICIN B and ITRACONAZOLE
Antifungals to be given in mycosis caused by mucor, rhizopus etc
3) What are the postulated reasons for a sudden apparent rise in the incidence of mucormycosis in India at this point of time?
Ans
Mucormycosis, colloquially known as black fungus, is a serious fungal infection that was seen in far smaller numbers in India before Covid-19, too. But it is now affecting post-Covid patients in large numbers. As of May 22, the government has reported 8,848 cases of this fungal disease, which can lead to serious complications and has a high rate of mortality.
Thus far, this surge has been attributed to the improper use of steroids to treat Covid-19 patients, coupled with poorly managed diabetes. But steroids in themselves are not the villains.
“Systemic (oral and intravenous) corticosteroids have been proven to reduce mortality in Covid-19,” Lancelot Pinto, consultant pulmonologist at Mumbai’s Hinduja Hospital, told Quartz. “The largest trial, Recovery, which proved this beyond a reasonable doubt among individuals who had low oxygen levels, used them in a dose of 6 milligrams Dexa per day for up to 10 days.”
Not only in Covid-19, but steroids are also widely used in orthopaedic and pulmonary diseases. In India, the problem lies not in the drug but in how it is prescribed. “Most of us who work in India will agree that prescribing practices more often than not tend towards higher doses for longer periods of time, which is a clear risk factor for invasive fungal infections,” Pinto said. Added to this, there is no strict prescription check in India, and most drugs—even those that need a prescription—can be easily bought over-the-counter.
“In addition, India has an epidemic of type 2 diabetes, and a significant proportion of patients with diabetes are diagnosed late in the illness,” which, according to Pinto, could be contributing to this surge in cases.
INFECTIOUS DISEASES COVID-19
1) Covid 19 with co morbidity (Pulmonology/Rheumatology)
1) How does the pre-existing ILD determine the prognosis of this patient?
Ans
the covid infection is more severe and extensive in people with pre existing lung disease
2) Given the history of autoimmune disease in the patient, how does the administration of steroids for COVID affect her RA and hypothyroidism?
Ans
3) Would this patient have an increased risk for post covid autoimmune response compared to patients without a history of autoimmune disease?
Ans yes
4) Why was she prescribed clexane (enoxaparin)?
Ans
It is a prophylactic measure in order to prevent any coagulation as covid-19 is a hypercoagulable state.
2) Covid 19 with Diabetes
Link to the patient case report log:
1) Since patient didn't show any previous characteristic diabetes signs, did the Covid-19 infection aggravate any underlying condition and cause the indolent diabetes to express itself? If so what could be the biochemical pathways that make it plausible?
Ans
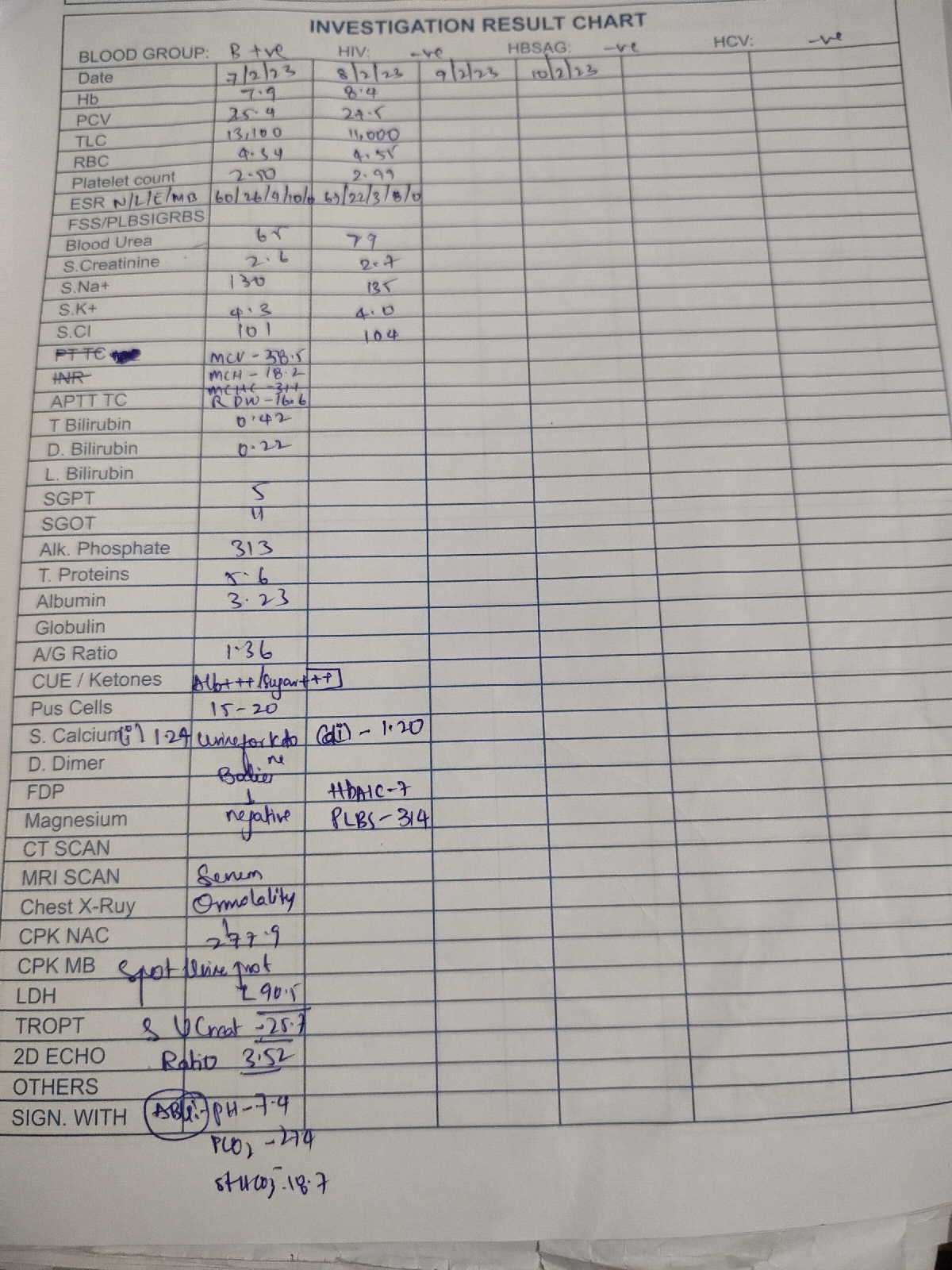
Her HbA1C is 7.9 which means that she was having raised sugar from long time,it might have been diagnosed while performing routine diagnostic tests.
2) Did the patient's diabetic condition influence the progression of her pneumonia?
Ans
Diabetes ia a metabolic disease which might significantly influence pathologic processes in body.
3) What is the role of D Dimer in the monitoring of covid? Does it change management or would be considered overtesting?
Ans
D-dimers are the indicator of thrombosis.In severe covid, the pathologic events lead to vichows triad and hence monitoring and carefully evaluating the patients for thrombotic events is necessary.
3) Covid 19 Severe
Link to the complete case report log:
1. Why was this patient given noradrenaline?
Ans
the patient suffered kidney failure which lead to persistent hypotension for which noradrenaline was given
2. What is the reason behind testing for LDH levels in this patient?
Ans
increase in LDH always denotes some sort of damage
here, increased LDH levels was relatable to some sort of damage in his body
3. What is the reason for switching from BiPAP to mechanical ventilation with intubation in this patient? What advantages did it provide?
Ans
BiPAP is a positive pressure system which has failed in this patient and for improving O2 saturation more invasive method which pushes air directly into lung was needed
4) Covid 19 Mild
Link to the case report log:
Questions:
1. Is the elevated esr due to covid related inflammation?
Answer:
Yes, as ESR is an important indicator of immunological loss, and as there is an increased inflammation and immunological dysfunction in COVID, elevated ESR is most likely due to COVID related inflammation.
2. What was the reason for this patient's admission with mild covid? What are the challenges in home isolation and harms of hospitalization?
Answer:
duration of infection was very high
SOB was grade 3
the above 2 factors were the reason for his hospitalisation
challenges for home isolation
- inadequate precautions
- no social distancing
- no monitoring
- emotional trauma for family
PROBLEMS WITH HOSPITALIZATION
- high cost
- stress to patient
- risk of infection to visitors
- over testing.

{kind=link}
{kind=link}
{kind=link}